Osteogenesis imperfecta pedigree: inheritance, germline mosaicism and lethal OI counselling
A clinical guide to reading and counselling from an osteogenesis imperfecta pedigree — autosomal dominant COL1A1 and COL1A2 genetics, the contribution of recessive forms, and the textbook two-neonate germline mosaicism case.
Short version. Osteogenesis imperfecta (OI; ICD-10 Q78.0; OMIM 166200 and related) is a group of collagenopathies, with the common types I, II, III, and IV caused by dominant-negative or haploinsufficient variants in COL1A1 or COL1A2. Autosomal dominant inheritance is the rule for the common types; a small minority of cases are autosomal recessive. Type II OI is perinatal lethal and has a high de novo rate. The textbook counselling scenario — two consecutive lethal OI pregnancies from unaffected parents with the same pathogenic variant — updates the posterior probability of parental germline mosaicism to approximately 99% and the recurrence risk for a subsequent pregnancy to approximately 13%. This is the clinical case where the true recurrence risk only becomes apparent at the second affected pregnancy, and it is why OI sits at the centre of germline mosaicism teaching.
Osteogenesis imperfecta: clinical overview and types
Osteogenesis imperfecta is a heritable disorder of connective tissue characterised by increased bone fragility, variable short stature, blue sclerae, dentinogenesis imperfecta, and adult-onset conductive or mixed hearing loss. The Sillence classification divides the collagen-based forms into four types:
- Type I: the mildest form. Normal or near-normal stature, blue sclerae, variable fracture frequency (usually a reduction after puberty), typical life expectancy, and sometimes adult-onset deafness. Caused most often by null alleles of COL1A1.
- Type II: perinatal lethal. Multiple intrauterine fractures, severely short limbs, beaded ribs, markedly reduced chest size with pulmonary hypoplasia, and death in utero or in early infancy. High de novo rate; dominant-negative COL1A1 or COL1A2 variants are typical.
- Type III: the most severe non-lethal form. Multiple fractures at birth, progressive deformity, severe short stature, dentinogenesis imperfecta, and wheelchair dependence in many cases.
- Type IV: moderate severity. Short stature, variable fracture frequency, often normal sclerae, and dentinogenesis imperfecta in some patients.
Beyond the classical Sillence types, a growing list of OI-like disorders arise from defects in post-translational modification of collagen (CRTAP, P3H1/LEPRE1, PPIB), chaperone and folding function (SERPINH1, FKBP10), bone mineralisation (BMP1, TMEM38B), signalling (WNT1, CREB3L1, SPARC), and others. Most non-collagen OI forms are autosomal recessive and therefore change the pedigree counselling materially from the dominant-model default.
Management is multidisciplinary. Bisphosphonates (pamidronate, zoledronate) remain the mainstay of pharmacological therapy, reducing fracture rate and improving bone density. Emerging antibody therapies targeting sclerostin and transforming growth factor-beta are in trials. Orthopaedic surgery (intramedullary rodding), rehabilitation, dentistry, and hearing management are essential. Genetic counselling is a cornerstone, both at diagnosis and at each subsequent reproductive decision.
COL1A1 and COL1A2 genetics
COL1A1 (17q21.33) and COL1A2 (7q21.3) encode the alpha-1 and alpha-2 chains of type I collagen, which assembles as a heterotrimer of two alpha-1 chains and one alpha-2 chain. Two distinct mutational mechanisms produce OI:
- Haploinsufficiency — typically null alleles of COL1A1 that reduce total type I collagen quantity. Clinical phenotype is usually mild (type I OI).
- Dominant-negative — missense variants, typically glycine substitutions in the triple-helical Gly-X-Y repeats, that incorporate into the heterotrimer and destabilise the entire molecule. Clinical phenotype is usually moderate to severe (types II, III, IV).
The key counselling fact is that an affected individual with an autosomal dominant COL1A1 or COL1A2 variant transmits the variant to 50% of offspring, each of whom is expected to manifest the condition with high penetrance. For type II perinatal lethal OI, the proband typically does not survive to reproduce, so the pedigree usually consists of an isolated affected fetus or neonate born to unaffected parents — either a de novo event or parental germline mosaicism. For type I OI, vertical transmission across multiple generations is common, and the pedigree often shows multiple affected individuals with variable severity, driven by modifiers and by stochastic fracture exposure.
The autosomal dominant calculator produces per-individual affection probabilities given the pedigree structure; see that page for the underlying arithmetic.
The two-neonate counselling dilemma
The clinical case that anchors OI teaching is this: an unaffected couple has a pregnancy with prenatally or neonatally identified perinatal lethal OI. Molecular testing of the neonate identifies a pathogenic variant in COL1A1 or COL1A2. Parental testing on blood is negative for the variant with adequate sensitivity. The couple is counselled that the event is likely de novo, with a small residual recurrence risk driven by unobserved parental germline mosaicism — typically in the 3% to 8% range depending on assumptions. The couple proceeds to a second pregnancy, which is also affected by perinatal lethal OI with the same pathogenic variant.
At the second affected pregnancy, the Bayesian update is sharp. Two independent de novo events in the same couple's gametes producing the identical variant would be astronomically unlikely. Parental germline mosaicism, by contrast, elegantly explains both pregnancies: one parent's oocyte or sperm lineage carries the variant at some fraction, and two independent conceptions drew affected gametes. The posterior probability that one parent is germline-mosaic rises to approximately 99%. The recurrence risk for a third pregnancy is commonly counselled at approximately 13% — reflecting the transmission probability weighted by the expected germline fraction conditional on two prior affected pregnancies.
A pedigree example
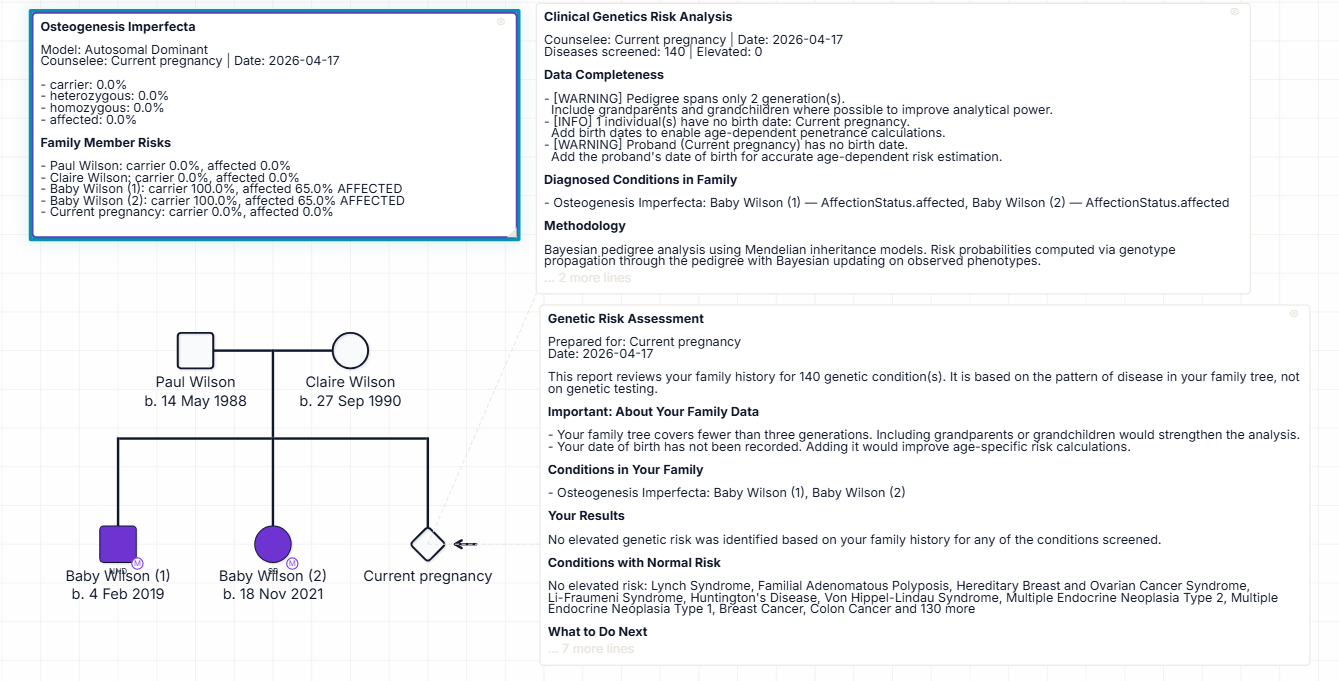
The pedigree above shows the classic two-neonate OI counselling case. An unaffected father and an unaffected mother have had three pregnancies. The first two pregnancies ended in perinatal lethal OI, both drawn as filled symbols with a slash to indicate deceased status, and both annotated with the same COL1A1 or COL1A2 pathogenic variant. The third pregnancy is the current one, drawn as a circle/square with a question mark or a "P" annotation to indicate ongoing pregnancy. Parental testing of blood is negative for the variant in both parents with appropriate deep-sequencing sensitivity.
Read the pedigree as a sequence of Bayesian updates. Before the first pregnancy, the prior probability of parental germline mosaicism was at the population prior (approximately 0.2% for OI). After the first affected pregnancy, that prior is updated but modestly. After the second affected pregnancy, the posterior concentrates strongly on the mosaicism hypothesis (~99%) because no other explanation fits as cleanly. The current pregnancy inherits that posterior: recurrence is approximately 13%, and prenatal testing at CVS or amniocentesis, or preimplantation genetic testing in future pregnancies, becomes a central part of the counselling plan.
The sex of the mosaic parent is often not identifiable from pedigree structure alone. Sperm sequencing in the father, and, where feasible, targeted deep sequencing of maternal blood or surrogate germline tissue, can refine the estimate and identify the mosaic parent. Where sperm VAF is measurable, the recurrence estimate can be calibrated directly from the germline fraction.
Prenatal counselling and reproductive options
Counselling priorities in the OI mosaicism case:
- Anchor the recurrence estimate transparently. Explain the two-neonate update, the approximate 13% recurrence, and the assumptions — particularly the mosaicism prior used and the sensitivity of parental blood testing.
- Offer targeted parental deep sequencing. Blood deep sequencing in both parents can detect somatic-germline mosaicism; sperm sequencing in the father directly estimates the germline fraction for paternal-origin mosaicism.
- Discuss prenatal testing in the current pregnancy. Chorionic villus sampling in the first trimester, or amniocentesis in the second, can test fetal DNA for the familial variant with the same sensitivity as proband testing. Results return in time to inform continuation-of-pregnancy decisions.
- Discuss preimplantation genetic testing for subsequent pregnancies. With a known familial variant, preimplantation testing for monogenic disorders (PGT-M) is technically straightforward; success rates depend on embryo number and clinic.
- Support the psychosocial weight. A second lethal pregnancy in a couple who had been counselled at low recurrence is emotionally formidable; the counselling style should explicitly name this and offer appropriate support.
For the broader germline mosaicism literature and the joint-parent posterior calculation, see our germline mosaicism calculator guide.
How Evagene supports osteogenesis imperfecta pedigrees
Osteogenesis imperfecta is a first-class catalogue entry in Evagene. The record carries ICD-10 Q78.0, type-specific OMIM identifiers including 166200 (type I), 166210 (type II), 259420 (type III), and 166220 (type IV), autosomal dominant inheritance for the common types with separate parameters for the recessive forms, type-specific de novo rate priors (with type II carrying a particularly high prior), and a germline mosaicism rate parameter around 0.002 that updates sharply in the face of multiple affected pregnancies. Annotating the proband with the correct OI type automatically exposes the correct parameter set to the analysis surface.
The autosomal dominant calculator handles the transmission arithmetic for multi-generation type I OI families with variable penetrance. The germline mosaicism posterior handles the lethal OI two-neonate case with joint-parent modelling, optional blood and sperm VAF inputs, and sensible priors. The output is a calibrated recurrence estimate with its assumptions surfaced, which is exactly what the family needs to understand before the next reproductive decision.
AI-assisted clinical interpretation using bring-your-own-key Anthropic Claude or OpenAI GPT models generates a structured report for the case, covering the OI type, the molecular result, the inheritance pattern, the germline mosaicism posterior, prenatal and preimplantation testing options, and the management plan for any affected pregnancy carried to term. For the broader rare-disease workflow see our rare disease pedigree software page, and for worked pedigree examples across inheritance patterns see our pedigree chart examples collection.
Frequently asked questions
What is the inheritance pattern of OI?
Most common types (I-IV) are autosomal dominant and caused by COL1A1 or COL1A2 variants. A minority of cases are autosomal recessive (CRTAP, P3H1, LEPRE1, and others). Type II is usually dominant with a high de novo rate.
What is the two-neonate counselling case?
Two consecutive lethal OI pregnancies from unaffected parents with the same variant. The posterior probability of parental germline mosaicism rises to approximately 99% and recurrence rises to approximately 13%.
Why is germline mosaicism so prominent in OI?
Because the phenotype is obvious in utero or at birth, type II has a high de novo rate, and recurrence reaches clinical attention at the second affected pregnancy. OI is among the cleanest empirical settings where mosaicism drives clinical decisions.
What are the Sillence types?
Type I mild; type II perinatal lethal; type III severe non-lethal; type IV moderate. Molecular classification now supplements the Sillence scheme, especially for non-collagen recessive OI.
What is the recurrence risk after a single lethal OI pregnancy?
Typically 3% to 8%, driven by unobserved parental germline mosaicism rather than the classical 50% dominant figure. After two affected pregnancies, approximately 13%.
Can prenatal testing help?
Yes — chorionic villus sampling, amniocentesis, or preimplantation genetic testing once the familial variant is identified.
How does Evagene handle OI?
OI is a first-class catalogue entry with type-specific parameters. Autosomal dominant inheritance, joint-parent germline mosaicism posterior, and AI interpretation run directly on the pedigree.